Say this 3 times fast… “Tricuspid Annular Plane Systolic Excursion”
At the last EDE 3, Dr Andrea Unger presented the parasternal short axis view and some newer Cardiac EDE concepts. Tricuspid annular plane systolic excursion was one of them, a term which I am hard-pressed to remember! Its acronym, TAPSE, is easier to recall, but Andrea wisely renamed this entity as “Base Jump”. While working on the POCUS database, I came across this article:
This was a substudy of the larger PROTECT study. The goal was to evaluate the relationship between TAPSE and clinical outcomes in normotensive patients with acute PE.
Methods:
Inclusion criteria:
Adults with acute PE diagnosed by CT within 14 days of symptom onset.
Exclusion criteria:
Given lytics
Hemodynamically unstable
Life expectancy < 3 months
Renal insufficiency
Pregnant
Unable to follow-up
All enrolled patients had a TTE performed by cardiologists looking for signs of RV dysfunction, including TAPSE on A4C.
Study outcomes:
All-cause mortality at 30 days, secondary outcome was PE-specific mortality
Results:
782 patients were included (66 others were removed due to incomplete TTE documentation, those excluded did not differ in terms of demographics, past history, clinical presentation). All were anticoagulated.
TAPSE range was 0.9-4.0 cm, with a median of 2.0 cm. ROC Curve analysis showed that the best cut-off for PE was 1.6 cm. 146 of the 782 patients had a TAPSE of < 1.6 cm. These patients were older, less likely to be male, had a higher prevalence of chronic heart disease or AFib, and more signs of clinical severity (syncope, tachycardia, low sats, hypotension [Editor note: presumably only brief episodes of hypotension since a normal blood pressure was required for inclusion]). 35 patients died by 30 days, 10 from a PE and 25 from something else. In 12 deaths, the TAPSE was less than or equal to 1.6 cm. 5 of these 12 deaths were from a PE. Both all-cause and PE-related mortality was significantly higher in those with a TAPSE < 1.6 cm. A low TAPSE was an independent predictor of death, even when patients with prior cardiopulmonary disease were excluded. On multivariate analysis, of all the echo features for RV strain, only TAPSE and the RV/LV diameter ratio were significantly associated with PE deaths. The Last Wave:
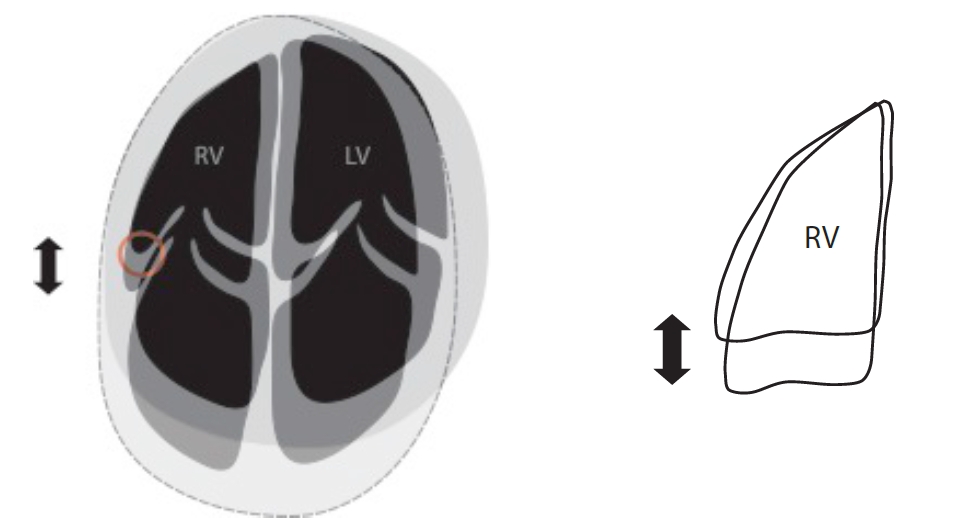
We will be adding TAPSE to the features of RV strain that we teach at EDE 2. In our experience so far, it is a useful adjunct that can usually be “eyeballed” to help decide if there is evidence of strain. See below for one of Andrea’s figures from EDE 3. It illustrates where to look for TAPSE and observe for the “Base Jump”.