


Stop missing biliary colic
 Editor’s note:
Editor’s note:
We’ve talked about the gallbladder before. And we will be talking about it again because the message needs to get out there. I will go out on a limb and state that it is still common for patients to present with epigastric pain that was previously diagnosed by the primary care physician or one of my colleagues in the ED as gastritis or “abdo pain NYD” and turns out to be biliary colic. Probably happens about every third shift for me, including my last one.
Conversely, I often get handovers at shift change waiting for their biliary scan in radiology. With a one minute look I can visualize a normal gallbladder and get the patient home or look into alternate diagnoses.
And yet I still get a lot of apathy or pushback about learning to scan the gallbladder. Sigh.
I can only believe those that often see abdominal pain patients are overconfident or delusional when they tell me that they see no use for doing bedside biliary scans. It is the atypical presentations and the fact that abdominal pain has so many potential aetiologies which should persuade everyone to get with the program. You will surprise yourself sometimes and save an unnecessary workup and delays in appropriate patient management.
Lloyd Gordon presents a recent case:
This patient in the early 40’s came in with central substernal chest
pain radiating directly to the back. Her history didn’t really consist
of much else. It had been there for a day or two. She was seen the day
before and sent home. Physical examination was also not enlightening.
She definitely was uncomfortable and had a lot of difficulty even
moving about on the stretcher. All the labs came back later normal.
Her IVC was pretty normal so no reason to give much IV fluid.
 Various views of her heart were pretty normal.
Various views of her heart were pretty normal.

I was checking the LKKS and noted this on the R lateral view.
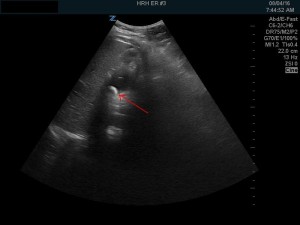
It certainly looked like a big gallstone impacted in the neck of the
gallbladder.
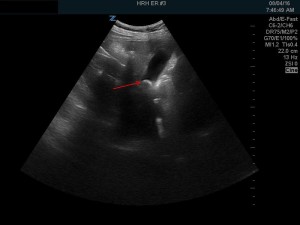
Views from the RUQ supine and in the left decubitus position confirmed this.
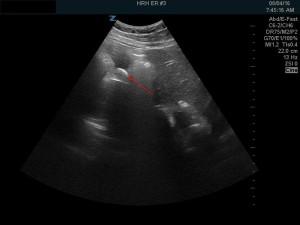
Of course, 10% of people have gallstones. However in all 3 views the
stone appeared to be impacted and immobile in the neck of the
gallbladder. Thus it was very likely the cause of her pain.
Referred to Surgery and operated later in the day.
The previous EP was younger, better trained, probably smarter than me
and yet didn’t make the diagnosis. The difference was POCUS.
Editor: And there you have it. Watch a tutorial video, take a course, learn how to do this scan quickly and safely. It does take practice but it’s a game changer, even for some of us older, less bright docs!


