



Yes, yes you do have time to do POCUS!
I was recently at the North York Emergency Medicine Update in Toronto, Ontario. An excellent emergency medicine conference, often the largest annual meeting of its type in Canada. During an amazing talk one of the plenary speakers, who loves ultrasound a lot, made a comment about rarely using it for nerve blocks. Why? Because it just takes too long.
Well the systems design part of me had a whole lot of disagreeing to do with that statement. You have time to do a block. You just haven’t prepared your department to do them.
Let me give you a little analogy and pretend you came from another place where medicine had evolved differently.
You never learned to do suturing of lacerations in residency but picked it up in some post-graduate workshops. Only you and a few other enthusiasts practice it in your ER. The nursing and allied staff aren’t all that familiar with it so they don’t know what to stock or prepare.
There are no laceration carts, trays, or rooms set up for doing suturing. Every time you want to repair a laceration you have to run to the four corners of the department gathering supplies. Some may have to be obtained from the OR because your department doesn’t stock them regularly.
You have no rooms or lighting to accommodate doing lac repairs so you have to do a lot of moving things around.
You may have to do extra explaining to staff and patients about what you are going to do because it’s rarely done in the ER. Most of your colleagues just call a surgeon who will do the repair in another department in a few hours during sociable hours and try to hold anything after-hours that is noncritical until the next day.
Guess how many lacerations you would be repairing in this system? How long would it take? Would it be good patient care to let the patients wait for delayed repairs?
That, my friends is where most of us are with POCUS guided procedures. You don’t have the prepared procedures trays. You don’t have the ultrasound machine properly set up ahead of time by staff. You don’t have the needed equipment and supplies properly stocked and available. You don’t have the experience of doing the procedure often enough to iron out all the small obstacles making it slow and inefficient.
What you have, is a system not designed to support POCUS.
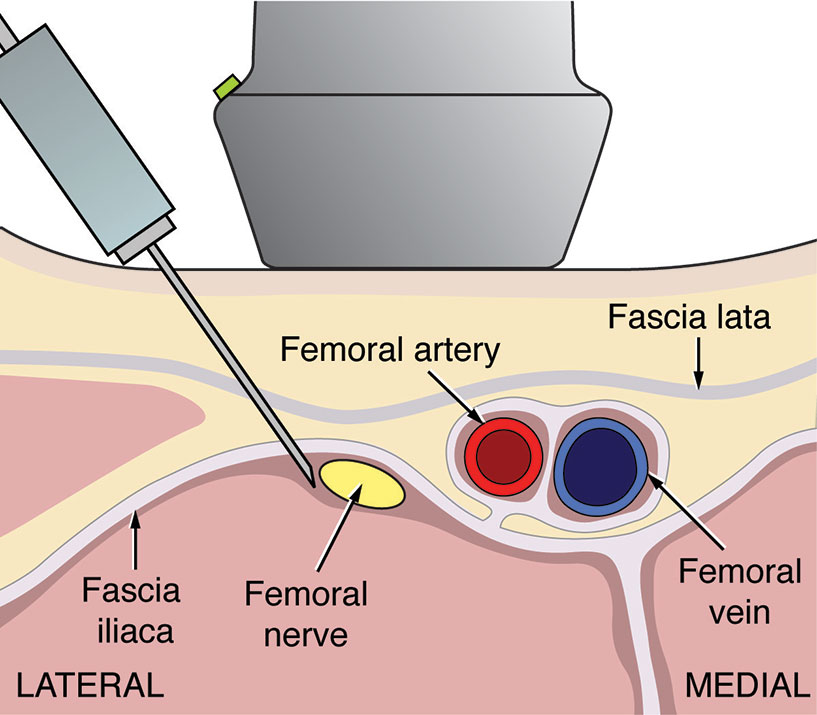
I have many stories of patients with femur fractures that were loaded up with opiods and miserable. Two children crying quietly while waiting to go to surgery. A horse-rider screaming with every move made to get him over for his XRays after a bad fall. A femoral block took the pain AWAY for all of them. The children relaxed and laughed with their families. The equestrian could get comfortable getting X-rays and waiting for his orthopaedic consult. This is the care I want for my fracture. One of my orthopaedic surgeons replied to my request to block his patients while waiting for surgery: “I hope if it’s my mother that comes into the ER next week you do a block.”
POCUS provides a valuable tool in multimodal pain control. There is growing literature demonstrating how it improves the acute care and long term outcome for many of our patients. You need to do more than master the skills of generating images and guiding needles with ultrasound. You need to look at creating a system to support this service. If there is one thing we can offer any patient in the ER, it is adequate pain control. You owe it to your patients to learn US guided regional anesthesia and to create a system to support this modality so you actually have the time to do the block.
Some reasons why you should do blocks now:
Impact of Ultrasound-Guided Femoral Nerve Blocks in the Pediatric Emergency Department
Don’t forget an earlier post of Steve’s on putting together a femoral block tray.



Great post Greg! Abolishing pain is perhaps the most important thing we can do for our patients in the ED, especially kids. Here are 3 more nerve block references for your readers that we will discuss on an upcoming EM Cases podcast episode on Peds POCUS with Jason Fischer, Alyssa Abo, Adam Sivitz & Alex Arroyo.
Frenkel, O., Mansour, K., & Fischer, J. W. J. (2012). Ultrasound-guided femoral nerve block for pain control in an infant with a femur fracture due to nonaccidental trauma. Pediatric Emergency Care, 28(2), 183–184
http://www.ncbi.nlm.nih.gov/pubmed/22307191
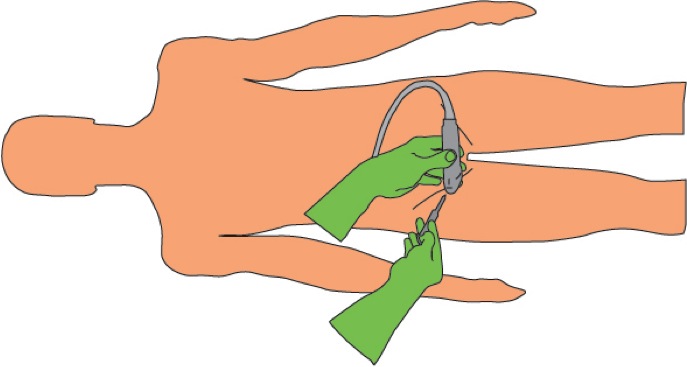
Liebmann, O., Price, D., Mills, C., Gardner, R., Wang, R., Wilson, S., & Gray, A. (2006). Feasibility of forearm ultrasonography-guided nerve blocks of the radial, ulnar, and median nerves for hand procedures in the emergency department. Annals of Emergency Medicine, 48(5), 558–562.
Herring, A. A., Stone, M. B., Fischer, J., Frenkel, O., Chiles, K., Teismann, N., & Nagdev, A. (2011). Ultrasound-guided distal popliteal sciatic nerve block for ED anesthesia. The American Journal of Emergency Medicine, 29(6), 697.e3–5.