



The Power of POCUS with clinical change
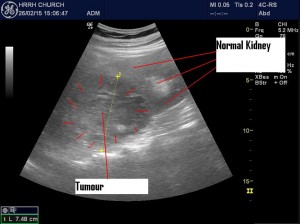
Do you ever feel your POCUS is unnecessary or somehow not as good as the “formal” ultrasound? I sort of wondered what I was going to find as this patient had been to hospital a number of times recently with 2 recent ultrasounds. Probably nothing to find? Well think again. She was able to localize her discomfort to the LLQ, so that was a start. First look at the kidney. I did a double take as it was abnormal (after 2 normal reports recently). There was a huge mass replacing most of the left kidney. I ordered a CT for the Urologist and referred the patient.
Here’s the original CT (the day of my POCUS). Of note is that the patient had had documented UTI’s with Klebsiella pneumonia (Res. Amp.) over the 4 months prior to my POCUS. She had been treated with Cipro/Septra on 2 occasions and Cetriaxone on another when a blood culture was positive (same Org./same Sens.)  The final path. diagnosis a month later was: acute and chronic pyelonephritis with cultures positive for K. pneumo. again, this time Res. to Amp and Intermed. Res. to Cefazolin. So it was actually a huge abscess secondary to recurrent pyelonephritis! Also her urine culture on the same day as my POCUS was + for E. coli ESBL Res. Amp/Cip/Sept but no Klebsiella! Weird.
The final path. diagnosis a month later was: acute and chronic pyelonephritis with cultures positive for K. pneumo. again, this time Res. to Amp and Intermed. Res. to Cefazolin. So it was actually a huge abscess secondary to recurrent pyelonephritis! Also her urine culture on the same day as my POCUS was + for E. coli ESBL Res. Amp/Cip/Sept but no Klebsiella! Weird.
[Ed. note] This goes to show the enormous benefit real-time scanning offers our patients. I can imagine most of you would have had a hard time convincing radiology to do yet another ultrasound in someone with two recent normal scans. POCUS allows you to have a low threshold to scan and to repeat the scan with any change in clinical status, be it weeks, days, hours, or minutes.



How long was the interval between the previous ( normal ) US and this finding?
How can such a mass (or even a smaller one) be missed by a sonographer?
Hi Yousry,
Those are excellent questions and unfortunately due to patient confidentiality and medicolegal issues the author doesn’t feel it prudent to provide more specific information at this time.