



How often do you use POCUS?
Dr. Gordon shares the findings from just three recent ED shifts. There are many negative and indeterminate scans here but it provides a glimpse into how POCUS is included in the thought process for risk stratification and clinical decision making.
This patient complained of R flank pain. POCUS revealed a normal kidney, uterus and pelvis. Her GB had stones but there was no sign of cholecystitis and a negative Sonographic Murphy’s Sign. So the gallstones were just a red herring. Further exam revealed a positive bowstring and straight leg raising on the R side. So the diagnosis was most likely sciatica which fitted the history. No further imaging.
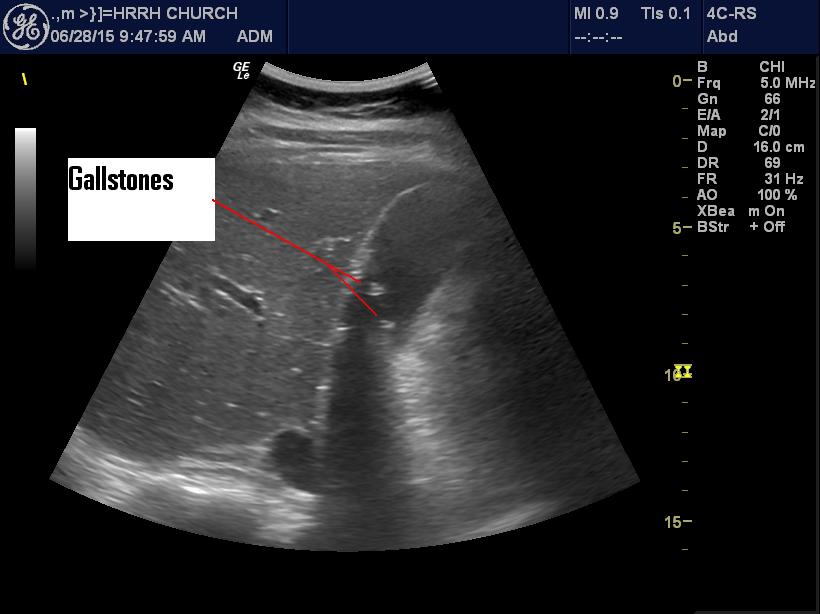
Asymptomatic gallstones
The next young woman had chronic recurrent abd. pain and she had it again. Nothing? However the RLQ revealed a suspicious area of fluid/oedema. A formal U/S showed appendicitis.

Two L Renal Colics in a row.
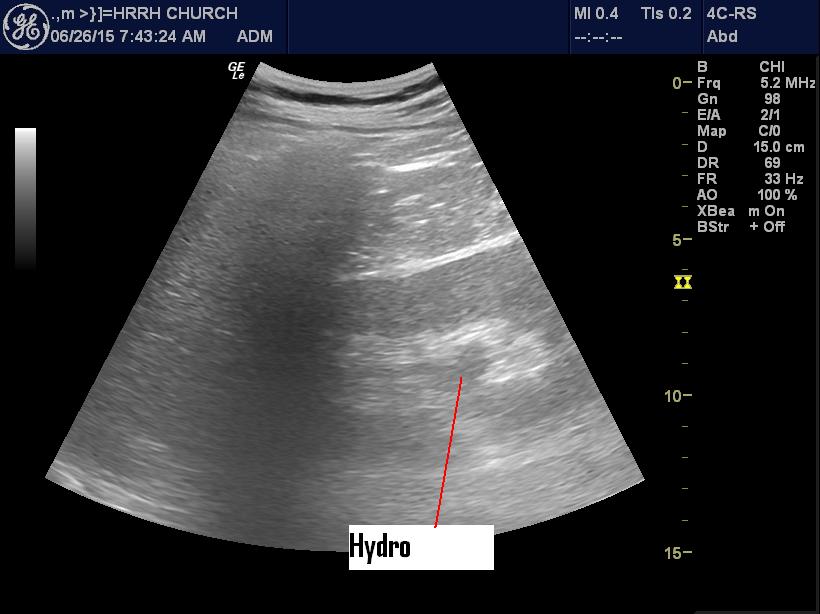
First Hydronephrosis patient

Second hydronephrosis patient
A red swollen umbilicus after cholecystectomy. POCUS revealed ab abscess.

Umbilical Abscess
This fellow had some vague abd pain. He was worried it was his umbilical hernia. The hernia was easily seen with POCUS and showed nothing but fat. When the patient pushed down I could see some fat (omentum?) sliding in and out freely. Not likely causing his pain.
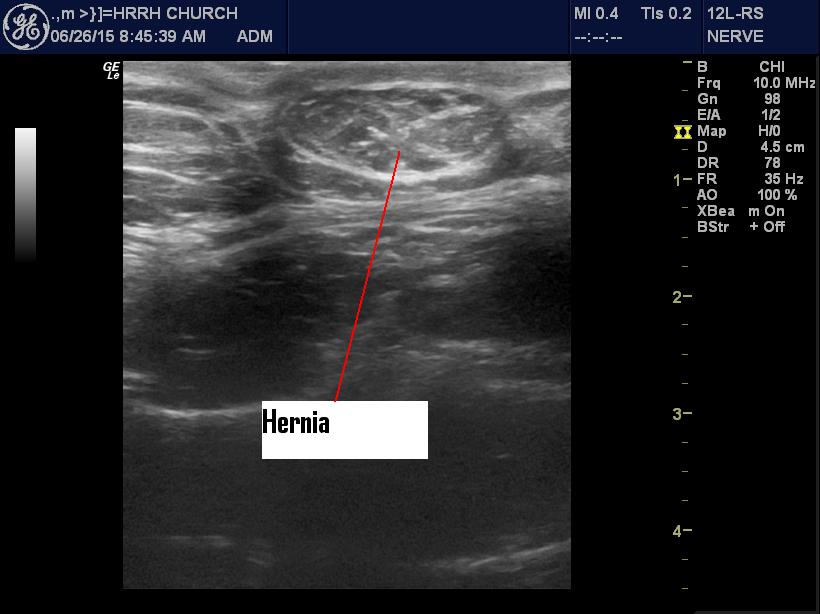
Umbilical hernia
This older man had a vasc. repair of his L Common femoral. The area was swollen and red. There was some serosanguinous fluid leaking out. POCUS revealed either an abscess or an organized hematoma. The graft could be seen below this with good flow (not seen in this picture.). No sign of leakage or flow outside the graft. Reassured that it was not likely a disaster, I still arranged for a Vascular consult that day.
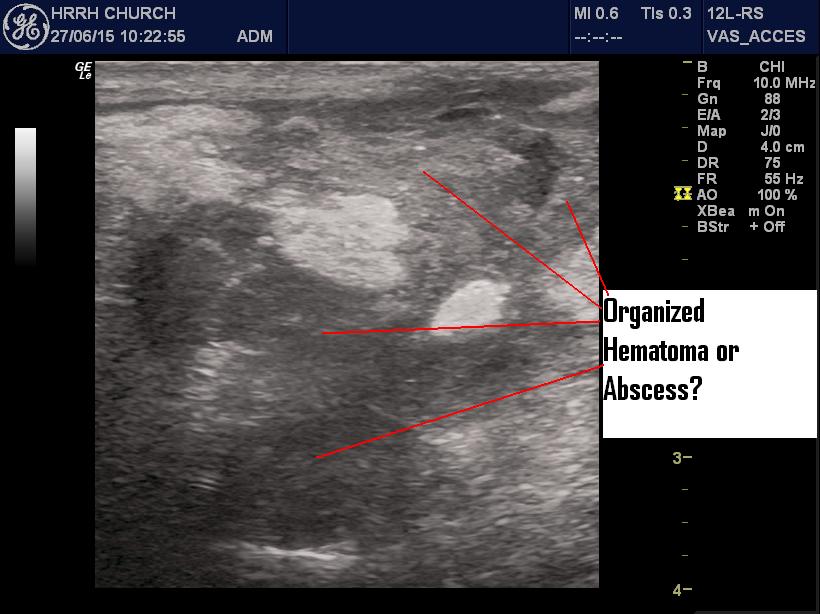
Hematoma?
A young man skated into the boards. Pain just posterior to the shoulder. POCUS revealed a scapular fracture.
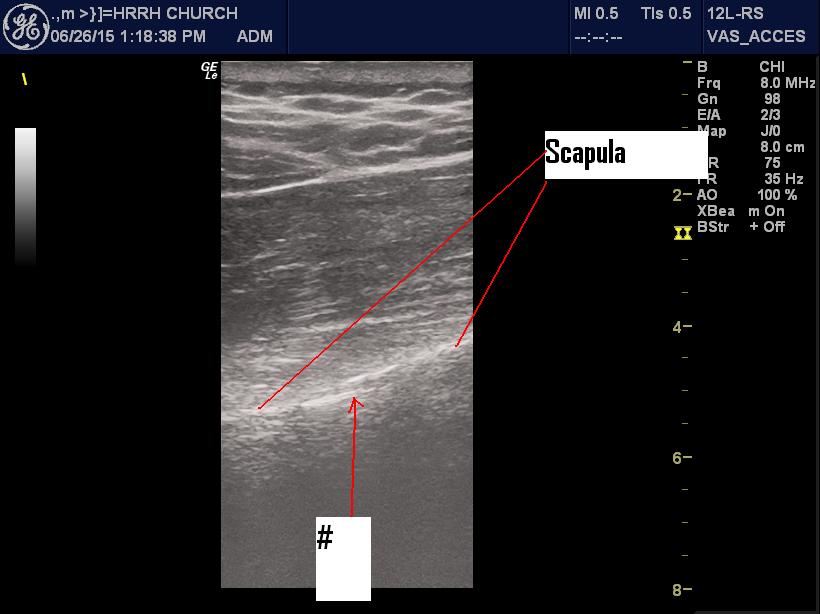
Right scapular fracture
This middle aged man had some odd epigastric pain. His abdominal aorta was a bit wide and I was worried that there might have been a thoracic aneurysm higher up.
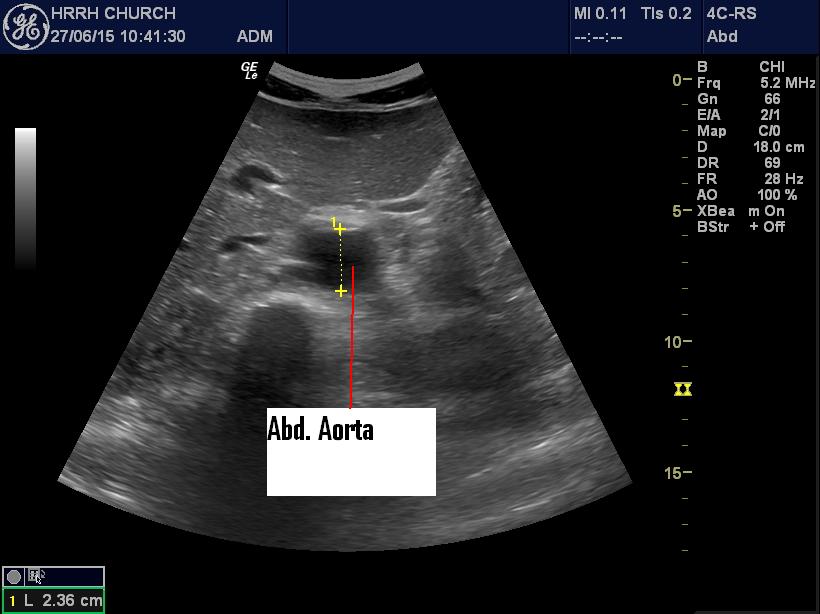
Normal abdominal aorta
I looked at the PSL view and could see the thoracic aorta was pretty much the same as below. Could still be a thoracic aortic aneurysm but this finding was re-assuring (+ a normal CXR).
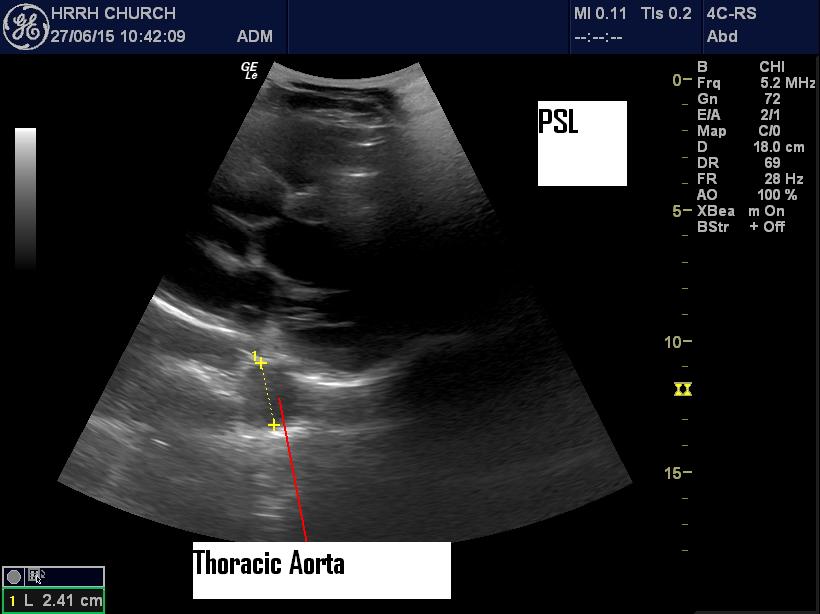
Normal diameter thoracic aorta
This 50’ish woman had a bad cough. Also a history of Rheumatic Heart Disease. Her O2 Sat was 95%. There were some adventitious sounds on the R. POCUS: I couldn’t get a great look at the atria but the ventricles looked Ok. The IVC was wide with little variation. There were no effusions. There were B lines on the R and none on the left. I ordered Avelox/Ventolin/Atrovent and just maintenance fluids. The CXR showed what I interpreted as a R pneumonia and cardiomegaly. The radiologist disagreed saying it was failure (with a large L Atrium). However with the unilateral B lines, I thought pneumonia was more likely. Of course with the RHD (Mitral Stenosis?), there was likely some component of chronic heart failure.
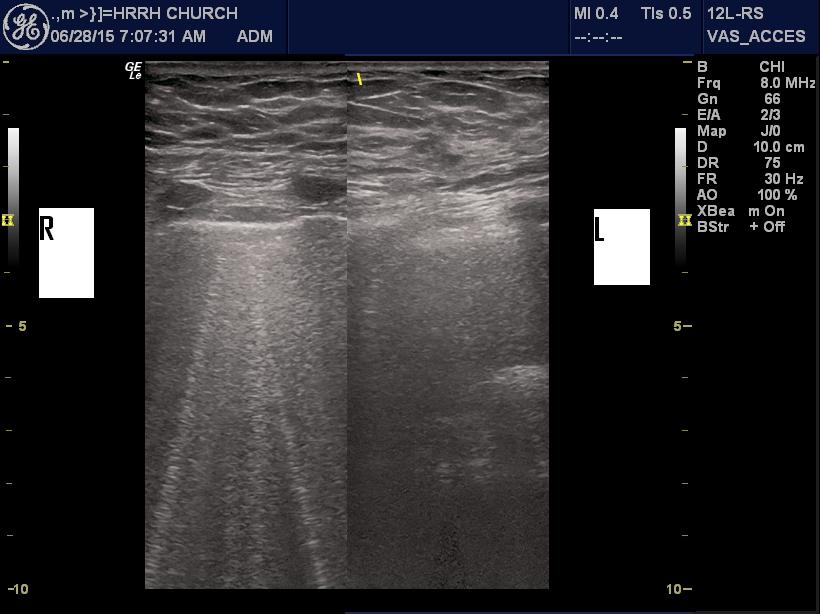
Pulmonary B-lines
A 2 year old with a swollen, red R scrotum and some R abdominal pain. Torsion? POCUS revealed bilateral hydrocoele R>L, an enlarged R testicle with excellent flow and a normal L testicle (flow not checked). Not sure what it was but not torsion. Referred to Urology in case it was an intermittent torsion.
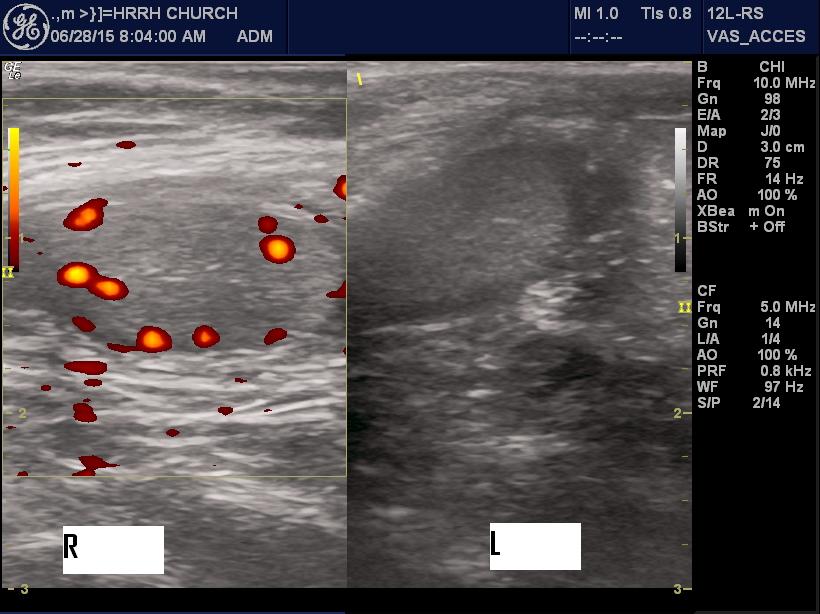
Testicles in 2 year old
This woman had a history of fever, generalized aches and pains, L flank pain, past renal stones and a sore throat (which looked completely normal). POCUS revealed a normal kidney with no hydronephrosis and great ureteric jets. I was still jittery about missing an infected, obstructing stone so I ordered a CT which of course was negative. Should’ve trusted the POCUS.

Normal ureteral jet
A young woman with L suprapubic pain and some vague urinary symptoms. She had a past history of SB resection for trauma. Her abdomen was pretty benign. POCUS revealed a normal L Kidney and a tender L Ovarian Cyst. The Small Bowel was normal looking with normal peristalsis. The MSU was full of WBC’s and + nitrites so I treated for UTI and advised her to have her GP follow up with an U/S in a couple of weeks.
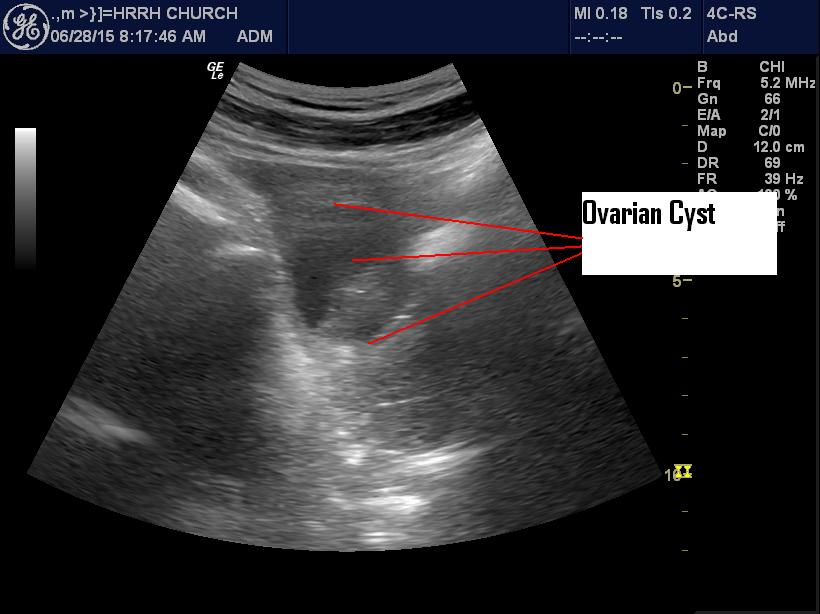
Ovarian Cyst
Last but not least was a very large elderly lady with lots of problems who came in with abd pain everywhere. She had a known large abd wall hernia on the R. It wasn’t tender but I didn’t seem to be able to reduce it. I was looking all over with the U/S and I sort of randomly found a dilated loop of SB > 3 cm. Aha! SBO with incarcerated hernia. Referred to General Surgery. The CT showed a SBO but not due to the hernia, maybe caused by adhesions. So much for Occam’s Razor.

Small Bowel Obstruction
There were lots more POCUS but mostly “boring” FAST’s, IVC’s, etc. Useful but getting to be old hat. I don’t know how people practise without POCUS. Sure you can do it, but why?


