



Appendicitis: It isn’t all about the size

During a recent EDE 3 course, I was asked about the cutoff size for appendicitis in children. I informed the learner that 6mm was the number I was taught to use for all ages. And this is certainly one of the most accurate measurements to use.
But this really doesn’t make sense in very young patients as the appendix grows significantly up to age 3 to 6 years. For those rare cases of appendicitis in small children, we are likely to miss it if we rely on size alone and the literature shows that the rate of missed and ruptured appendixes is high in this age group. In addition a lot of appendices are just not visualized well enough to do measurements. So what is our next move?
Ravichandran et al provide a great case of a 3 year old with a 5 mm appendix on ultrasound that was indeed appendicitis and discuss the need to look beyond 6 mm as the cutoff.
An important point is when looking for appendicitis, looking for secondary or associated signs will increase sensitivity for all comers. The appendix is just not that easily seen in almost 38% of pediatric patients. Radiologists know this and you will often read reports stating that the appendix was not seen but there were no secondary signs of infection making the diagnosis less likely (though not conclusive).
Estey et al in Pediatric Emergency Care looked at the predictive value of secondary inflammatory sonographic signs. They found large amounts of free fluid, phlegmon, and pericecal inflammatory fat changes were very specific for acute appendicitis.

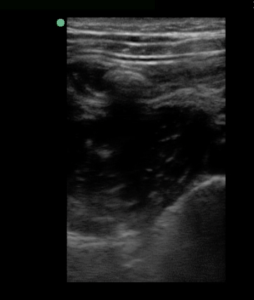
Acute appendicitis with inflammatory fat changes
Other associated signs to look for include fecolith, adjacent bowel hypokinesia, thickening of adjacent small bowel, enlarged mesenteric lymph nodes, and localized tenderness when compressing the iliac fossa. (Our GI ultrasound guru, Dr. Andrew Skinner, refers to this as the sonographic McBurney’s Sign.)
Fecolith
Overall, the specificity of secondary signs can be as high as 90%. So if the presentation fits, the appendix isn’t seen but secondary signs are present, there is a very good chance the patient has appendicitis.
But as Ross et al state in their review of clinical outcomes in appendicitis, if the clinical presentation is still concerning for appendicitis, the absence of secondary signs is not good enough to send the patient home as the sensitivity was only 40%.
So as always, use point of care ultrasound to help rule in the diagnosis and help rule it out in low pretest probability cases but for those with a concerning presentation and no alternative diagnosis, you can’t send them home if the appendix isn’t visualized and secondary signs aren’t present. Clinical judgement always supersedes your machine.
Just remember to look for those secondary signs and you might pick up a couple of appendicitis cases you might have missed otherwise.



Absolutely agree. Needs a little training though. I personally focus a lot on the appearance of the appendix layers especially the submucosa. An hypoechoic submucosa in a high probability pretest clinical setting is pretty specific for appendicitis even when the diameter is small.
Made this video collection on secondary signs: http://youtu.be/sm4M2H6SG04 (comments are in Italian though).